
Diabetic Ketoacidosis (DKA): High-Yield Guide for Physician Assistant Students

Diabetic Ketoacidosis (DKA) is a life-threatening complication of diabetes that requires prompt recognition and intervention. As a Physician Assistant Student, mastering DKA is crucial for your future practice. This high-yield guide provides you with the essential knowledge and skills to confidently diagnose, manage, and prevent DKA in your patients.
4.4 out of 5
| Language | : | English |
| File size | : | 439 KB |
| Text-to-Speech | : | Enabled |
| Enhanced typesetting | : | Enabled |
| Print length | : | 5 pages |
| Lending | : | Enabled |
| Screen Reader | : | Supported |
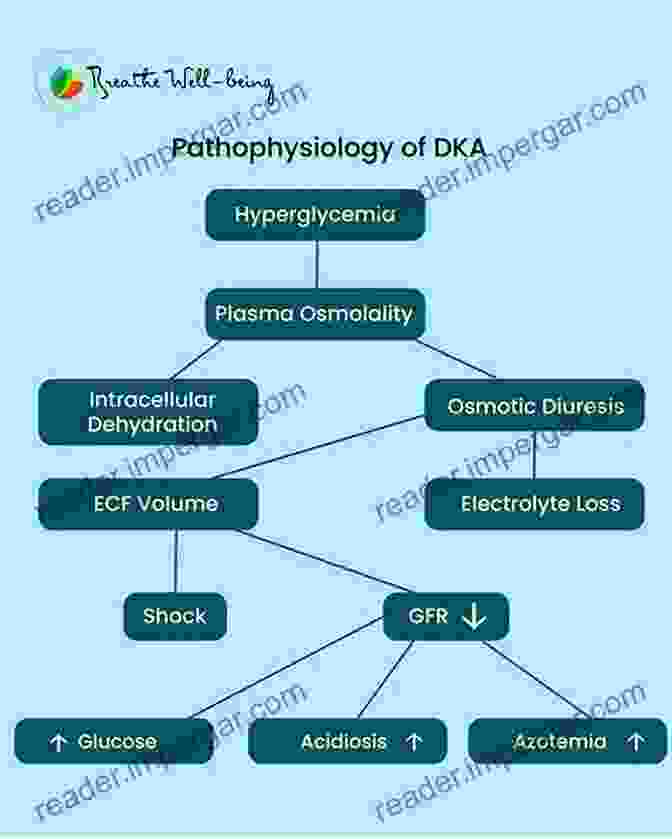
Pathophysiology and Clinical Presentation
DKA occurs when the body produces excessive ketones due to insulin deficiency or resistance. This can be caused by missed insulin doses, infection, trauma, or stress. Clinical manifestations include polyuria, polydipsia, dehydration, nausea, vomiting, abdominal pain, and a characteristic fruity breath odor.
Early recognition of DKA is vital to prevent severe complications such as cerebral edema, electrolyte imbalances, and sepsis.
Diagnosis and Laboratory Findings
Suspicion of DKA is based on the patient's history and physical examination. Laboratory testing confirms the diagnosis with elevated blood glucose (>250 mg/dL),ketonemia, and metabolic acidosis. Arterial blood gas analysis reveals decreased bicarbonate and pH, with an anion gap indicating ketoacidosis.
| Laboratory Finding | Normal Value | DKA Value |
|---|---|---|
| Blood Glucose | >250 mg/dL | |
| Serum Ketones | >3 mmol/L | |
| Arterial Bicarbonate | 22-29 mEq/L | |
| Arterial pH | 7.35-7.45 | |
| Anion Gap | 3-11 mEq/L | >12 mEq/L |
Other laboratory findings may include hypernatremia, hyperkalemia, and elevated creatinine.
Management of DKA
Management of DKA involves aggressive fluid resuscitation, insulin therapy, electrolyte correction, and monitoring of patient response.
- Fluids: Intravenous fluids (0.9% saline) are administered at a rate of 1-2 L/hour to correct dehydration.
- Insulin: Intravenous regular insulin is initiated at 0.1-0.15 units/kg per hour. This helps lower blood glucose and suppress ketogenesis.
- Electrolytes: Potassium and phosphate are commonly depleted in DKA and should be closely monitored and supplemented as needed.
- Monitoring: Patients require frequent monitoring of blood glucose, electrolytes, and vital signs. Arterial blood gas analysis is repeated regularly to assess the resolution of acidosis.
Case Studies
To further enhance your understanding, we present two real-life case studies that illustrate the presentation and management of DKA.
Findings: Blood glucose 350 mg/dL, serum ketones 4 mmol/L, bicarbonate 13 mEq/L, pH 7.25, anion gap 15 mEq/L.
Management: Intravenous fluids, insulin infusion, potassium supplementation, and frequent monitoring.
Outcome: Patient's condition improved gradually with resolution of acidosis and ketonemia within 24 hours.
Findings: Blood glucose 450 mg/dL, serum ketones 6 mmol/L, bicarbonate 10 mEq/L, pH 7.18, anion gap 18 mEq/L.
Management: Intravenous fluids, insulin infusion, antibiotics, and supportive care.
Outcome: Patient required mechanical ventilation due to severe acidosis. With aggressive treatment, his condition stabilized, and he was discharged after 5 days.
Mastering Diabetic Ketoacidosis (DKA) is essential for Physician Assistant Students. By understanding the pathophysiology, clinical presentation, diagnosis, and management of DKA, you can confidently provide safe and effective care to your patients. This high-yield guide provides the tools and insights you need to succeed in this critical aspect of diabetes management.
Don't miss out on this opportunity to elevate your knowledge and skills. Free Download your copy of Diabetic Ketoacidosis (DKA): High Yield for Physician Assistant Students today!
4.4 out of 5
| Language | : | English |
| File size | : | 439 KB |
| Text-to-Speech | : | Enabled |
| Enhanced typesetting | : | Enabled |
| Print length | : | 5 pages |
| Lending | : | Enabled |
| Screen Reader | : | Supported |
Do you want to contribute by writing guest posts on this blog?
Please contact us and send us a resume of previous articles that you have written.
 Book
Book Novel
Novel Page
Page Chapter
Chapter Text
Text Story
Story Genre
Genre Reader
Reader Library
Library Paperback
Paperback E-book
E-book Magazine
Magazine Newspaper
Newspaper Paragraph
Paragraph Sentence
Sentence Bookmark
Bookmark Shelf
Shelf Glossary
Glossary Bibliography
Bibliography Foreword
Foreword Preface
Preface Synopsis
Synopsis Annotation
Annotation Footnote
Footnote Manuscript
Manuscript Scroll
Scroll Codex
Codex Tome
Tome Bestseller
Bestseller Classics
Classics Library card
Library card Narrative
Narrative Biography
Biography Autobiography
Autobiography Memoir
Memoir Reference
Reference Encyclopedia
Encyclopedia Learn With Me
Learn With Me R C Morris
R C Morris Richard Smoley
Richard Smoley Leonard J Greenspoon
Leonard J Greenspoon Leah Wietholter
Leah Wietholter William Davison
William Davison Philippe Sands
Philippe Sands Kip Koehler
Kip Koehler Kinshasha Holman Conwill
Kinshasha Holman Conwill Louise Roberts
Louise Roberts Robert L Zimdahl
Robert L Zimdahl Kiri English Hawke
Kiri English Hawke Susan Conley
Susan Conley Karrine Steffans
Karrine Steffans Laura J Colker
Laura J Colker Laurie Ault
Laurie Ault Peter Allison
Peter Allison Leigh Gilmore
Leigh Gilmore Sussan Babaie
Sussan Babaie Paul O Jenkins
Paul O Jenkins
Light bulbAdvertise smarter! Our strategic ad space ensures maximum exposure. Reserve your spot today!

 Frank MitchellRevive Damaged Hair to Its Former Glory: A Comprehensive Beginner's Guide to...
Frank MitchellRevive Damaged Hair to Its Former Glory: A Comprehensive Beginner's Guide to...



 Leslie CarterFollow ·5.9k
Leslie CarterFollow ·5.9k William FaulknerFollow ·5k
William FaulknerFollow ·5k Shawn ReedFollow ·15.8k
Shawn ReedFollow ·15.8k Herman MitchellFollow ·7.1k
Herman MitchellFollow ·7.1k Bernard PowellFollow ·7.9k
Bernard PowellFollow ·7.9k Edward BellFollow ·4.1k
Edward BellFollow ·4.1k Derrick HughesFollow ·14.6k
Derrick HughesFollow ·14.6k Jim CoxFollow ·2k
Jim CoxFollow ·2k
 Gage Hayes
Gage HayesUnlocking the Secrets of History: The Republic of Laws by...
Delve into a Historical Masterpiece ...
 Chad Price
Chad PriceUnlock the Secrets of Voice Perception with the...
The human voice is a captivating and...
 Jon Reed
Jon ReedUncovering the Truth: The SADF and Cuito Cuanavale
The South...
 Eli Brooks
Eli BrooksAdaptations Of Literature And Fiction On The Airwaves: A...
The allure of literature and...

 Cason Cox
Cason CoxUnveiling the Past: A Comprehensive Guide to Modern...
History, the...
 Cormac McCarthy
Cormac McCarthy4.4 out of 5
| Language | : | English |
| File size | : | 439 KB |
| Text-to-Speech | : | Enabled |
| Enhanced typesetting | : | Enabled |
| Print length | : | 5 pages |
| Lending | : | Enabled |
| Screen Reader | : | Supported |
